
This is the second part of of the article which appeared as Part I on Tuesday 21 December 2021.
A study of 68 countries and 2,500 US counties, just published in the European Journal of Epidemiology, has just proved that vaccination rates are unrelated to COVID case numbers.
Remembering that there is much to be desired about the accuracy of the PCR test used to justify the lockups and the muzzling. Heavily vaccinated countries are having overwhelming surges in case numbers. Israel, which is exclusively Pfizer, by the way, and well into its booster program, Iceland, Ireland, the Seychelles, Gibraltar, the UK, and many parts of the states have high numbers. In fact, Waterford in Ireland has just announced the highest case numbers in the country in the face of a staggering 99.7% vaccination rate.
The study Shelton cites here has serious shortcomings, among which the most notable is that the authors conducted an ecological study among an undifferentiated population, and fallaciously came to conclusions at an individual level. The ecological fallacy is a favourite among antivaxxers, according to Dr David Gorski, an editor at Science-Based Medicine (a site I cannot recommend highly enough). Here’s another discussion of that particular fallacy in the context of Covid-19 by epidemiologist Gideon Meyerowitz-Katz.
Without running through all the countries Shelton names, it will suffice to examine the case of Israel, which he cites first, and is most often cited in this context. Here’s a great breakdown of why claiming a suspicious link between high vaccination rates and high infection rates is fallacious, and disappears as soon as you stratify the data by age and disaggregate it between vaccinated and unvaccinated.
Doing so shows that the vaccine was still highly effective in Israel in August, between 85% and 95% against severe disease, even with the delta variant in full swing.
No doubt the other nought 0.3% will be to blame. What are people saying? That my vaccine won’t work until you have yours? Really?
That is a terrifically puerile and obtuse argument for a doctor with 41 years under his belt. My vaccine will not produce herd immunity until you have yours, that’s true. Without you getting vaccinated, mine will have a decent, say 80%, chance of preventing serious disease and death, so if I happen to be in the unlucky one in five, your non-vaccination could harm me, yes. It could also harm people who, for medical reasons, cannot be vaccinated, and can rely only on herd immunity for protection.
Perhaps Shelton should leave the snide levity for occasions where it is merited.
In a recent hospital outbreak in Israel, 95% of the cases were fully vaccinated. The double vaccinated in Scotland now comprise 89% of the deaths from COVID-19 in a trend that has been increasing for months. According to the latest technical report from public health Scotland a month ago, the figure for England was 86%.
See ecological fallacy, above. Specifically, note that while the rate of severe cases is three times higher in the unvaccinated than in the vaccinated, the risk of severe disease is 20 to 40 times higher in elderly people. So, because elderly people are far more highly vaccinated than younger people, they will be over-represented in the data, creating the false impression that vaccination fails to curb hospitalisations or death.
As of yesterday in New Zealand, only 17% of new COVID-19 admissions to hospital were in unvaccinated people.
That may be so, but as of yesterday in New Zealand, only 6% of the eligible population was unvaccinated, and only 9% was not fully vaccinated. Assuming, then, that the hospital admissions were for the most part over the age of 12, the unvaccinated are two to three times over-represented in hospital admissions. I’m not sure that’s the case Dr. Shelton wanted to make, but there you go.
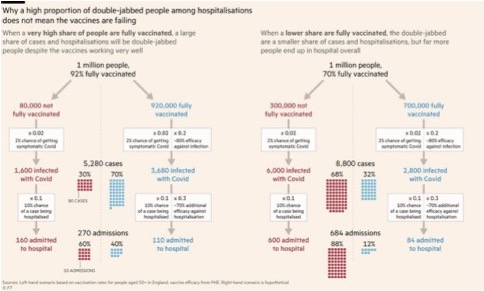
This is another schoolboy error, which once again calls into question Shelton’s ability to ‘assess data and understand the science’. Here’s a picture for him, courtesy of the Financial Times:
So the next time a social media influencer looks you in the eye and tells you that if you get the vaccine, you cannot die, please recognise disinformation.
What a crude straw man that is. That wouldn’t make it past a ninth-grade debating team. Nobody has ever said if you get the vaccine, you cannot die. I’m not sure insulting the audience’s intelligence is a good strategy, here.
But we must remember that the total deaths are still very small relative to total infections diagnosed by a PCR test, that multiple courts around the world, and even Dr. Fauci and the CDC admit is not fit for purpose. At the cycle threshold of 40 or above that is used here in New Zealand, most tests are false positives. Please remember that as the media spoonfeeds you the daily community case numbers.
This is a red herring. It is true that a PCR test alone cannot conclusively diagnose a SARS-CoV-2 infection. This is why it is used as a diagnostic aid, in conjunction with clinical symptoms. It is also true that high cycle thresholds can lead to high false positives, although Shelton’s claim of ‘most’ seems exaggerated.
Ultimately, however, people are treated based on their clinical presentation. They are hospitalised based not on PCR tests, but on symptoms. They are admitted to ICU, not based on their PCR test, but on their symptoms. And their death is classified, not based on their PCR test alone, but on their symptoms.
In fact, multiple studies have shown that cases aren’t being over-counted, but are being systematically under-counted. A February 2021 study in Plos One reckons there are five to 20 times as many cases as officially reported, in half of the countries studied. A PNAS study from August 2021 found a 60% under-count in the US. The Council on Foreign Relations also reports substantial under-counts in major countries around the world.
Our health authorities are refusing to let our doctors do what they are trained to do, including to do no harm with experimental drugs, but instead gets us before the New Zealand Medical Council if we speak out on any of these issues. At least two of us here are about to be suspended.
So far, Shelton and his motley crew seem to have plenty to answer for.
We continue to hear though from patients and clinicians, that CARM [Centre for Adverse Reactions Monitoring] reports of suspected harm are not being lodged.
That is a neat way to inflate the claims of ‘suspected harm’, but if claims of harm are not being lodged, that might well be because there are no claims of harm to lodge.
Remember these reports only require a suspicion, not proof, of vaccine harm and must be made if we are to pick up the signals.
Indeed, and because they only require suspicion, they most certainly overestimate the incidence of vaccine-related harms.
We find it deeply disturbing that the New Zealand Ministry of Health is forcing many thousands of health, education and other workers to take the shot, which has also produced many severe side effects, and we suspect may be linked to the deaths of over 250 new Zealanders and many more with life-changing injuries.
‘We suspect’. Considering that New Zealand has only had 49 deaths of Covid-19 (which makes it a remarkable outlier in the world), one has to suppose that the official response to the pandemic was wildly successful.
One would also imagine that 250 vaccine-related deaths would be the biggest story of the year. Yet I was able to find only two news reports of deaths that were believed to have been caused by vaccine side-effects: a 26-year-old man in Dunedin, and a woman in her 50s.
There’s another point to be made here. Fringe websites have published claims such as that more New Zealanders have died of vaccines than died of Covid-19. Let’s ignore that you’d have to count every post-vaccination death as a death caused by the vaccination for that to be true. Let’s suppose that is true.
When that claim was made, it involved 40 supposed vaccine-related deaths, compared to 27 deaths of (or as the antivaxxers like to say, ‘with’) Covid-19. The spectacular success of the New Zealand response to Covid-19 means that if the vast majority of the population of had not been vaccinated, the country would likely have seen thousands of deaths. (Applying the global crude mortality rate to the population of New Zealand produces about 3 500 deaths.)
Now, from a public health perspective, or a personal risk-benefit perspective, would even 40 vaccine-related deaths outweigh the 3 473 deaths of Covid-19 that were avoided?
As we learn about vaccine complications, it is clear that the difference between serious injury and death is pure luck for many people. Again, we challenge Medsafe [New Zealand Medicines and Medical Devices Safety Authority] to properly investigate, to please prove us wrong, instead of them hiding behind the claim of not enough information to assess.
I can’t answer for Medsafe, but I’m pretty sure they’re not covering up multitudes of vaccine-related injuries or deaths.
In an important paper from Queen Mary’s Hospital in London, researchers looked at a random group of reports to the Vaccine Adverse Effects Reporting System or VAERS in the US. They concluded it was only possible to rule out 14% of cases as definitively not caused by the vaccine on the provisional assessment, before detailed and expert assessment must then be undertaken.
Without a detailed and expert assessment, this is entirely meaningless. It is a little puzzling why someone from Queen Mary’s Hospital in London was looking at VAERS data, and not at their own Yellow Card system, but here it is.
It is an extraordinarily superficial assessment, which ruled out the vaccine as a cause of death only in people that were literally on their death beds already. In only 5% of cases did they consider the vaccine the most likely cause of death, which would translate to 82 vaccine-related deaths in total, in the entire US, out of 240 million people who have received at least one dose, and compared to 827 226 deaths of Covid-19 itself.
It is an unpublished, non-peer-reviewed paper, authored by an inexperienced post-doctoral researcher in computer and information science, a researcher in cognitive psychology, a lecturer in computer science and information technology, and a railway health and safety officer. Perhaps it’s not wise to take it as the final word on vaccine-related deaths in the US.
An proper analysis of deaths reported via the Yellow Card system in the UK is instructive. Out of 1 645 reported deaths, only the vaccine was determined to have been the primary cause in five cases, and the vaccine was a contributory cause in another four. Conversely, only one in 200 death reports to the Yellow Card system turns out to be vaccine-related.
Austrian pathologist Dr. Peter Schirmacher found that 60% of a series of consecutive post vaccine deaths that he autopsied were caused by the vaccine with findings never seen in any other condition. A team of German pathologists has validated his findings.
I could not source this to a medical journal, even though Schirmacher is a fairly prolific author on pathology. The newspaper article (Google translation) in which the claim does appear says Schirmacher is the chief pathologist at Heidelberg University in German, not Austria. It also says that of the 40 autopsies on which Schirmacher is reporting, ‘he assumes that 30 to 40 percent of them died from the vaccination’ (my emphasis).
So Shelton gets a lot of this wrong. So, it appears, did Dr. Schirmacher himself. His colleagues in Germany – far from ‘validating his findings’ – said that his statement was incomprehensible, and that such a conclusion could not be drawn from unreported data.
Dr. Jessica Rose, immunologist and computational biologist has a report on the CDC website detailing, by multiple different methodologies, the likely death rate to be at least 10 times the number reported to VAERS, which is currently about 18,000.
No such report exists on the website of the US Centers for Disease Control. Rose is a post-doctoral researcher at the Israel Institute of Technology, and together with antivax statistician Mathew Crawford authored a paper submitted to regulations.gov, a website that allows public comments on US government matters. It therefore has no more standing than the rantings at authority of random aggrieved nuts.
Reuters did a comprehensive fact-check of the paper, and concluded that its claims are false.
A variation of this talking point claims that, judging by VAERS reports, the Covid-19 vaccines are the deadliest vaccines ever made. They are not.
These systems are known to under-report, probably dramatically. And it is very likely that our CARM system is very under-representative of the true death and injury toll.
Speculation. Also, quite likely to be wrong. The Covid-19 vaccines have seen a remarkable increase in reports to adverse event reporting systems. This is often interpreted as evidence that these vaccines are more dangerous than previous vaccines.
However, there is an alternative explanation. First, this has been the largest and fastest vaccine rollout in history, by a country mile. This alone could explain the increased reporting levels.
Second, that this has been the most politicised vaccine rollout ever, with antivaxxers and right-wingers prominently and persistently agitating against, and warning of the dangers of vaccination, which would fuel adverse event reporting of dubious veracity.
We are not claiming to know with any certainty, but it is not our job. Our job is to raise concerns, and we expect our institutions to do their bit.
At least he is aware that he doesn’t know with any certainty.
Our government was earlier found guilty of breaching its own rules when they gave provisional consent for emergency use authorisation for the vaccine for the whole country. So it quickly changed the law.
This is true. A High Court ruling found that it was ‘reasonably arguable’ that the provisional approval of the Pfizer vaccine was ‘problematic’. That’s hardly a strong condemnation, but the New Zealand government changed the wording of the law that said any provisional authorisation should apply only to a ‘limited use’, which might have been read to preclude a widespread vaccination rollout in all adults.
Does that same cavalier attitude explain…
Speculation, and tendentious speculation at that.
…why the Medsafe CARM system is so lagging with its register of severe side effects and deaths linked to this vaccine?
Medsafe and CARM are being regularly informed via members of the New Zealand Health Forum as to their latest citizens database information, available on our website, and which is now including some children.
These heroic people are filling the gap that our health sector should be active in. What normal human would not want to investigate these possible cases. We are in a clinical trial. It is the time spent watching for effects that makes it so, not the number of doses given. Based on many testimonies from patients and healthcare workers, some of these are sworn legal statements. We can say confidently that our pharmaco vigilance is failing. In clinical trials of new medications, the drug is guilty until proven innocent.
I was unable to verify much of this. Although there was a single news article announcing the formation of the ‘Health Forum NZ’, it offered no link to its website. It does, however, seem to duplicate the functionality of another group, which seems strange.
A search failed to turn up a website for either New Zealand Health Forum or Health Forum NZ. A page that claims to offer access to the spreadsheet of post-vaccination deaths maintained by Health Forum NZ proved to be inaccessible.
That leaves only a closed Facebook group with over 50,000 members, which appears to be dedicated to soliciting anecdotal evidence from the general public about post-vaccination adverse events.
Given that a formal system for registering adverse events does exist, this seems like a superfluous exercise, and given the likely audience this is likely to attract, it seems like a biased exercise.
The latest official report on adverse events following vaccination in New Zealand can be found here (and newer reports will be published here). I don’t see any obvious problems with it.
The US alone is reporting, as I say, over 18,000 deaths on its system equivalent to our CARM, but multiple independent, highly qualified researchers are calculating figures many times higher.
We’ve discussed this.
Although some countries now seem to be stepping aside. It seems that there remains a lock-step coercion to jab and boost everyone over and over from cradle to the grave, …
That is a bit of an exaggeration. Yes, the most common policy is widespread vaccination, including children, in an attempt to reach herd immunity. Yes, many, if not most, countries have introduced booster vaccine shots to strengthen immunity, especially with the emergence of the latest variant, Omicron, which appears to be able to escape immunity derived both from prior infection and vaccination.
There is, perhaps, an argument to be made for whether vaccine rollout programmes should be complicated by recognising immunity from prior infection. This is, indeed a discussion in the medical literature, and some countries do recognise prior infections in their pandemic control policies.
However, Shelton neither makes a good case for it here, nor could one trust his bona fides if he were to make it.
…and discredit any other treatments with mountains of real-world evidence and that will save lives if given early to high risk patients. Taking paracetamol and throat lozenges and waiting to go blue is the official approach, apparently. Where is the duty of care from primary care?
He’s on about ivermectin again, isn’t he? Yeah, he is. As discussed above, the case against ivermectin.
The GP college says these early treatments can’t be used, but wait a little, and we expect to see a brand new patented clone of ivermectin approved and sold at huge expense to taxpayers sometime soon, who will also have to stump up for welfare payments to the huge pool of talented and dedicated and smart people now forced out of work by these mandates.
Merck’s molnupravir and Pfizer’s PF-07321332 are the two new drugs for the treatment of Covid-19. Presumably, Shelton is referring only to molnupravir, since Merck also manufactures ivermectin.
Neither drug is a clone of ivermectin. Neither drug is repackaged ivermectin. Shelton is dissembling. As a doctor, speaking on a public platform, he really ought to know better.
So now it’s the children’s term to experiment or not to experiment. Why is it even a question? If you believe that we should experiment on children, we can’t help you at this stage.
Nobody is ‘experimenting on children’. Vaccines for children have undergone full safety trials, just like the vaccines for adults, and no serious side-effects were detected.
Would Shelton rather not trial medicines for children, so we’d have no medicines for children? Of course he wouldn’t. He is just using emotive language in an effort to raise alarm among people who don’t really understand how medicines are developed.
‘Think of the children!’ is a clichéd rhetorical ploy that replaces reason with emotion in a debate. It has been described as an ‘ethics fallacy’.
Ironically, not vaccinating children could just as easily be described as an experiment. It is too early to tell, but initial signs are that the latest variant, Omicron, could cause more severe disease in children than previous variants did. If we don’t curb the spread among children, we will fail to control the spread of the virus.
Protecting children against disease by vaccination does not constitute ‘experimenting on children’.
Kids and unborn babies have their whole lives ahead of them for problems to manifest and to pay the price for our recklessness.
They would also ‘pay for our recklessness’ if we did nothing, and they became orphans, or they contracted multisystem inflammatory syndrome from Covid-19 infection.
Shelton wove another misconception into this line, which is that the vaccines might have serious long-term consequences that have not been detected yet. This is a common antivax trope, but it has no basis in science or history.
There has never been a side-effect of any vaccine in history that was not triggered within six weeks of administration. There isn’t a plausible mechanism by which such long-term side-effects might occur, either, since all vaccine components are fully metabolised within weeks of administration.
Reliable figures are emerging, putting children’s risk of serious harm from the jabs to be at least 10 to a hundred times greater than from the infection itself.
Children are even less likely to come to harm from COVID than from the flu. The incidence of heart inflammation from the vaccine is much greater than we first thought. And the Pfizer clinical trial did not have anywhere enough children to produce meaningful results.
This line of reasoning appears to trace back to the comments of Michael Yeadon, a former Pfizer executive turned antivax hero.
This is the same guy that said: ‘Viruses do not do waves. That’s just a myth based on poor understanding of influenza at the end of WW1, a century ago.’
This is the same guy that in October 2020 said: ‘The pandemic is effectively over.’
For a detailed assessment of the risk/benefit of Covid-19 vaccination to children, given the low risk of myocarditis, this is an excellent article. Although there is some dissent, the near-universal conclusion, given the available evidence, is that even in young people, the benefits of vaccination far outweigh any harm, and the risks of being unvaccinated are far greater than any rare side effects from the vaccines.
The British Medical Journal reported by the way last week on irregularities, mismanagement and fraud from the main trial. But this news has not been covered by the media, and we’re not aware that our authorities have questioned Pfizer on this.
It did. Contrary to Shelton’s claim, it was covered widely by the media.
The allegations made in the report have not been proven. Even if they were, ethics expert Simon Kolstoe, writing for The Conversation, says: ‘Given the size of the vaccine trial, and the many centres involved, bad data from a few rogue centres is unlikely to fatally undermine the evidence needed for licensing the Pfizer vaccine.’
The author of the report did not bother to contact the contracting firm allegedly involved in the misconduct, but it told Kolstoe: ‘Ventavia is aware of recent accusations in an article written by Paul Thacker [investigative reporter and author of the BMJ article]. Mr. Thacker did not contact Ventavia prior to publication. These same accusations were made a year ago, at which time Ventavia notified the appropriate parties. The allegations were investigated and determined to be unsubstantiated. Ventavia takes research compliance, data integrity, and participant safety very seriously, and we stand behind our work supporting the development of life-saving vaccines.’
Kolstoe concludes: ‘Given the vast amount of funding, and thousands if not millions of researchers working on COVID, alongside the successes there will inevitably be more examples of alleged misconduct – leading, inevitably, to sensationalist headlines. But when this happens, it is important to remember how many lives the vaccines and other treatments have saved. Yes, science is a human activity. Yes, integrity can be a problem. Yes, fraud and misconduct will occasionally occur, but science also produces remarkable results.’
Indeed, even if the entire Pfizer trials were to be overturned (and that is vanishingly unlikely), they have been superseded by evidence of safety and efficacy from literally billions of vaccine recipients around the globe.
Dr. David Gorski, writing for Science-Based Medicine, points out examples of deliberate exaggeration and misrepresentation in the article, and he leaves out key information. Gorski notes: ‘Everything about Thacker’s article frames the clinical trial and Pfizer in the worst possible light. It’s almost as though the report is custom-made to provide grist for antivax conspiracy theories, and it definitely succeeds at doing just that.’
Gorski concludes that the article is evidence of smoke, but not fire, and goes on to describe warning signs about the British Medical Journal itself in his very lengthy analysis of the case.
We believe ongoing mountains of shame should be felt by anyone who contributes to coverups. And we now await legacy media’s messaging that it is common for children to have heart attacks and strokes, and that the troubling rise in death rates of people under 50 occurring in most vaccinated countries is some sort of mystery.
This ‘troubling rise of death rates’ among the vaccinated is not something you’ll find in respectable media. You will, however, find it in tabloids and on antivax sites. All of them are variants on the observation that all-cause mortality among young people is higher in 2020 than in 2021. This is then attributed to vaccination, and not, for example, to the emergence of the Delta variant. The claim that all-cause mortality is higher among the vaccinated is another example of the ecological fallacy we saw above: because older people and people with comorbidities are more likely to be vaccinated, they will of course have higher all-cause mortality than younger, healthier, but unvaccinated people.
This is another case of searching for statistics that appear to support a preconceived argument, creatively misinterpreting them, and then generalising from the results.
Check out proper journalists like Mike Whitney and Alex Berenson on Denmark, Germany, Ireland, and Israel who are all reporting troubling rises.
Alright, let’s check them out.
Mike Whitney is a freelance photographer, who reckons Covid was a bioweapon made in the US and aimed at China, and that the conspiracy theorists were right, it is a ‘Poison-Death Shot’.
Alex Berenson is a former New York Times reporter who now gigs around on alt-right media spreading Covid-19 misinformation, earning the high accolade from Derek Thompson in The Atlantic as ‘The Pandemic’s Wrongest Man’.
If these are the ‘proper journalists’ on which Dr. Matt Shelton relies for his information, it’s no wonder he is so comprehensively wrong on almost everything.
And listen to the Western Australian premier. His hospitals are chokka. It ain’t Covid. And he’s very worried about why.
The premier of Western Australia, Mark McGowan, has said that hospitals in his state, but also other states, are under pressure ‘no-one has ever seen before’. He says it is hard to know why it is, except that ‘there is some evidence that it is some sort of delayed reaction to Covid’.
Two months earlier, emergency doctor and Australian Medical Association spokesman David Mountain told Australia’s ABC News that the health crisis was not a result of Covid-19, but of underinvestment in the system, in the face of an aging population.
The state’s health minister, Roger Cook, disagreed, claiming there was a pandemic-related spike in hospital demand.
McGowan also blamed the federal government, saying that there are a significant number of people who are in hospitals that should be managed by the National Disability Insurance Scheme, or should be in aged care.
All states and territories have since requested additional funding from the federal health minister, Greg Hunt.
Mere days later, Cook challenged Australia’s prime minister, Scott Morrison, who said the stresses on hospital systems in some states had ‘nothing to do with Covid-19’, saying that there has been a significant increase in demand as a result of Covid-19, mainly as a result of increased mental health presentations and people deferring care from 2020.
Of course, antivaxxers are pointing the finger at vaccinations, even though there is absolutely no evidence for such a claim.
In conclusion, we will continue to try to lobby government and health agencies on behalf of our people, and our profession, whilst fending off their campaign of suppression and intimidation.
You do that, mate.
Thank you for your attention.
No, thank you.
The views of the writer do not necessarily reflect the views of the Daily Friend or the IRR.