
One of the go-to alternatives for people who for some absurd reason are hesitant about Covid-19 vaccinations is the anti-parasitic drug ivermectin, the evidence in favour of which has gone from weak to non-existent.
In fear and desperation, people will try anything. That explains a great deal of so-called ‘alternative medicine’, especially for intractable or incurable conditions such as arthritis or cancer.
Of course, as the legendary Tim Minchin pointed out, ‘Alternative medicine has either not been proved to work, or been proved not to work. Do you know what they call alternative medicine that’s been proved to work? Medicine.’
In 2020, faced with a deadly pandemic, people were desperately casting about for cheap and effective cures. I can’t count the number of ‘protocols’ I’ve come across, recommending everything from vitamin supplementation to colloidal silver. They were usually concocted not by specialist virologists, but by general practitioners with demanding clientele and a more ‘holistic’ persuasion than a scientific education ought to have inculcated.
Many of these protocols include ivermectin, a bold defence of which was recently penned in these pages by Andrew Kenny.
Ivermectin has been unjustly denounced as ‘horse dewormer’. It is, but it is also approved for use in humans for its anti-parasitic properties against nematodes (worms) and arthropods. It is indicated for use in cases of scabies, river blindness, strongyloidiasis, ascariasis, trichuriasis, lymphatic filariasis, and lice. It is also believed to have anti-bacterial and anti-viral properties, although the research on this is scant and emerging.
Cochrane review
A recent Cochrane Review of studies on the use of ivermectin for the treatment or prevention of Covid-19 is instructive. Its conclusion: ‘Based on the current very low‐ to low‐certainty evidence, we are uncertain about the efficacy and safety of ivermectin used to treat or prevent Covid‐19. The completed studies are small and few are considered high quality. Several studies are underway that may produce clearer answers in review updates. Overall, the reliable evidence available does not support the use of ivermectin for treatment or prevention of Covid‐19 outside of well‐designed randomized trials.’ (My italics.)
The reason I refer to this Cochrane Review is that it is easy to be misled by outlier studies, or apparent anomalies, or studies that appear to a layman to be good, but aren’t, or studies that are misinterpreted by people with an agenda. A comprehensive review of studies conducted by a reputable organisation trumps all the show-and-tell pizzazz of the average anti-vax, pro-ivermectin website.
The evidence for ivermectin’s use is weak and contradictory. Interest was sparked by an Australian study in which ivermectin was demonstrated to work against a range of viruses, in the lab, and in doses far higher than humans could tolerate.
As a scientist once quipped, if they handed out Nobel Prizes for diseases we could cure in the lab, we’d all have one.
Retractions
Several of the most widely cited studies supporting ivermectin use in humans against Covid-19 have been retracted due to fabricated data and scientific fraud.
The most recent retraction is of a Lebanese study (the Retraction Watch website is temporarily down, hence the archive link). A large study conducted in Egypt was retracted in July, and another from Argentina, which claimed an unprecedented-in-the-history-of-medicine 100% efficacy in preventing Covid-19, and was promoted by populist anti-vaccination luminaries such as Bret Weinstein, has also come under withering fire from experts, including in this thread by epidemiologist Dr Gideon Meyerowitz-Katz.
After the latest retraction, Meyerowitz-Katz’s meta-analysis of randomised controlled trials of ivermectin shows a marginally negative effect:
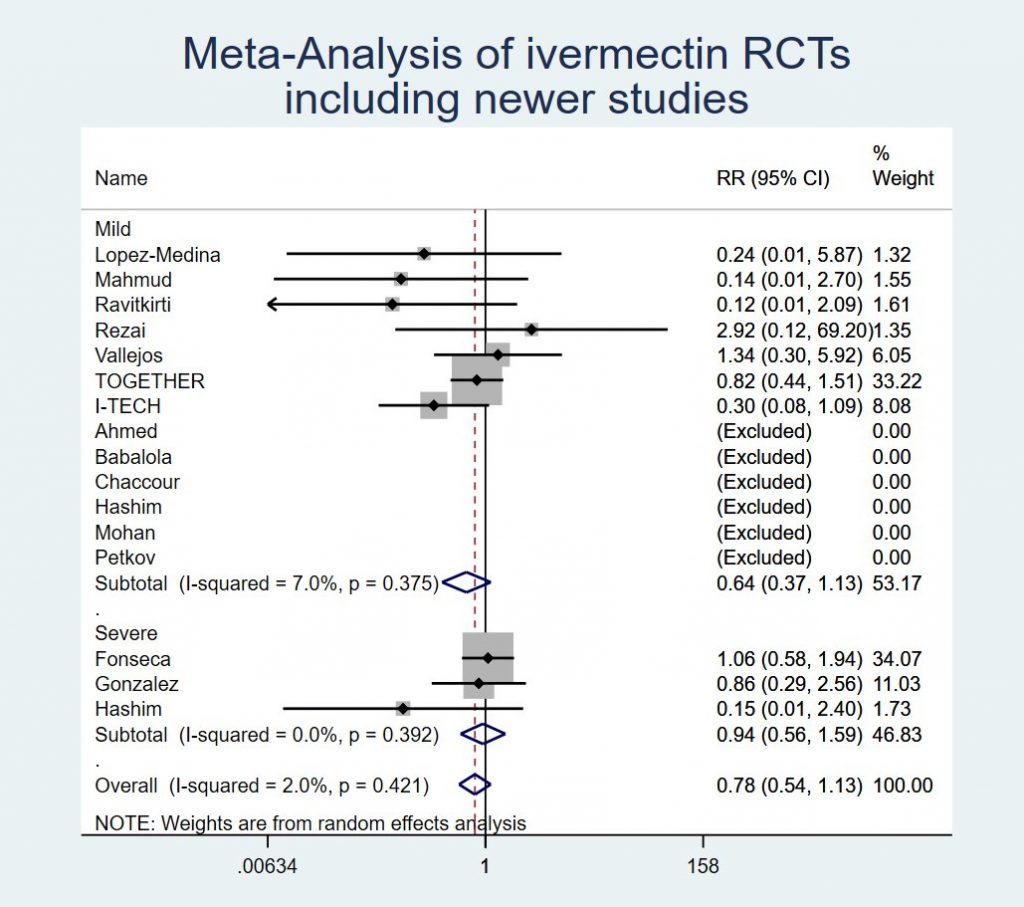
Not only has the effectiveness of ivermectin for the treatment of Covid-19 not been demonstrated, but neither has its safety. For all its conventional uses, ivermectin is given in one or, rarely, two doses. For preventing Covid, it needs to be taken regularly and for a long time.
There are no safety tests for long-term, frequent ivermectin use. Nor are there studies that assess what the correct dosage ought to be for prophylaxis, early treatment of Covid, or treatment of severe Covid, so proponents of ivermectin are literally guessing at what dosage to recommend.
With the massive increase in ivermectin use by lay people to prevent or treat Covid-19, it isn’t surprising, then, to find reports of toxic effects and overdoses. It might be safe, in appropriate doses, but there is no good evidence that proves that it is.
There really isn’t any good evidence that ivermectin is a particularly useful drug in the fight against Covid-19, let alone that ivermectin treatment or prophylaxis is a reasonable alternative to vaccination.
Misconceptions
Let’s refer back to Mr. Kenny’s article to clarify a few more misconceptions commonly held by ivermectin pushers. (I’ll render his words in bold italics, for convenience.)
‘There is now a demented war against a very safe, cheap drug…’
No, no there isn’t. There is a rational, considered, scientific review of the evidence, and a rejection of poor research and fraudulent studies. This is neither demented, nor is it a war.
‘Evidence shows it [Covid-19] might have been engineered in the Wuhan laboratory in China.’
Actually, it doesn’t. There is no good evidence either way. It could have been leaked from a lab by accident. It might have been engineered in a routine gain-of-function experiment. But there is no conclusive evidence for these assertions.
‘To get emergency authorisation for their use, the health authorities needed to know there were no alternative treatments.’
This is only a guideline. The guidance for emergency use authorisation (EUA) says: ‘The Commissioner may issue an EUA to allow an MCM to be used in an emergency to diagnose, treat, or prevent serious or life-threatening diseases or conditions caused by a CBRN agent when there are no adequate, approved, and available alternatives.’
There were no adequate, approved, and available alternatives. Ivermectin is not a vaccine, so it is not an alternative to a vaccine. Ivermectin had not been approved for use either as a prophylaxis or a treatment against Covid-19. Ivermectin had not completed clinical trials for use against Covid-19. Ivermectin was being used on a purely experimental basis outside the US.
Even if ivermectin worked as a prophylaxis, taking chronic medication with potential harmful effects on the liver and kidneys is no adequate alternative.
Conspiracy
‘Ivermectin, developed by Merck in 1980, might well have been such an alternative. But it was now out of patent, and very cheap. The vaccines could make huge profits for the drug companies; Ivermectin could not. The vaccines were granted authorisation.’
Here is the setup for the conspiracy, which is developed further in the article.
If this were how the pharmaceutical industry worked, however, I’d be quite baffled by the fact that the first-line antipyretic and analgesic given in hospitals is not some expensive, patented super-drug, but little old 19th-century paracetamol: unpatented, generic, and dirt cheap. I’d be equally baffled that the first-choice treatment for Covid-19 includes dexamethasone, a very cheap drug in plentiful supply around the world.
Let’s suppose, for a moment, that the conspiracy is true. That is, Merck recommended against using ivermectin for Covid-19 because it had been given a grant by the US government to help develop an anti-viral drug effective against Covid-19 (which is had), and that it was basically repackaging ivermectin in a shiny new capsule under a shiny new name to sell it for a fortune.
Why would the Food and Drug Administration (FDA) tolerate such blatant profiteering? Well, perhaps the FDA is in the pockets of Merck.
But then, why would the South African Health Products Regulatory Authority (SAHPRA), play along?
Why would the same socialist government that once went to war against the capitalist pharmaceutical companies over AIDS drugs (and so set the precedent for overriding pharmaceutical patents), now suddenly conspire to enrich those very same pharmaceutical companies, instead of choosing widely available and inexpensive alternatives?
If ivermectin worked, it would have been an absolute election gift to the ANC. Like the ANC, it doesn’t work, sadly.
Mr. Kenny himself points to a second inconsistency with the conspiracy theory: why would the woke left-wing media, like The Guardian, have defended Merck for recommending against ivermectin? They’re no friends of the pharmaceutical industry, either.
And no, the drug that Merck eventually developed (and is indeed selling for a fortune) is not just dressed-up ivermectin.
VAERS
Here are some further issues I have with Mr. Kenny’s piece.
‘They [vaccines] seem to have done much more good than harm, although they have proved by far the most dangerous vaccines of the last thirty years, as can be seen in the USA Government’s Vaccination Adverse Event Reporting System (VAERS).’
They have certainly done more good than harm. In fact, they have done very little harm indeed. Serious side effects have been exceedingly rare.
Using VAERS reports as a measure of relative harmfulness is misguided, however. Never in the history of medicine have so many people been vaccinated in such a short space of time. Never in the history of medicine has a vaccine been so politically controversial. Never in the history of medicine has the anti-vaccine movement been so loud. And never in the history of medicine have so many people had internet access to make VAERS reports.
These factors alone can explain why the number of VAERS reports involving Covid vaccines far exceeds the reports for previous vaccines.
VAERS reports can be made by anyone. They do not need to be verified. There does not have to be a causal connection, or any connection at all, with the vaccine, other than that it won’t let you report an adverse event that happened prior to vaccination. (I know, I tried.)
Post hoc, non ergo propter hoc (after this doesn’t mean because of this) applies to every VAERS report. At best, such reports are grounds for further investigation. What they are not, is a basis for making any sort of claim about the frequency of adverse events caused by a vaccine.
One extremely rare side-effect of Covid-19 vaccines (or rather, of the J&J vaccine specifically), is blood clots in women. Here’s how the risk equation works out:
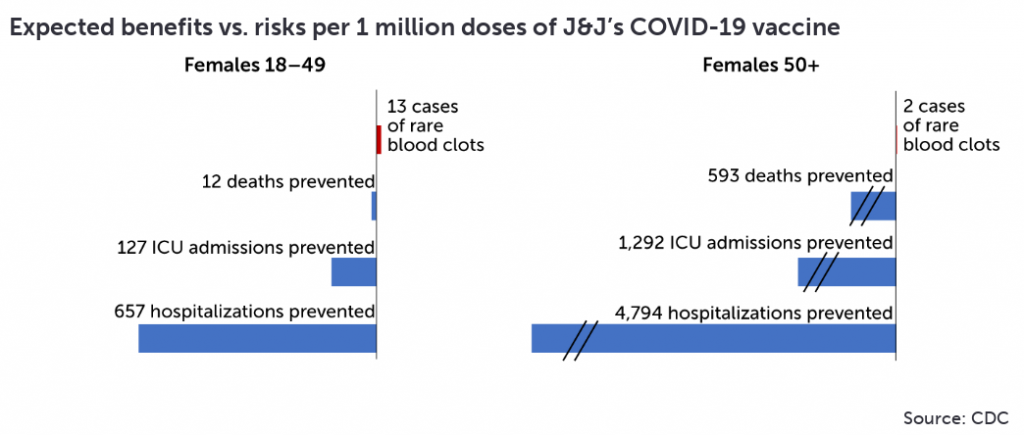
A similar case can be made for heart inflammation, which is easily treatable. Even among young vaccinees, where the relative risk of heart inflammation is highest, and the risks of Covid are the lowest, the benefits of vaccination outweigh the risks.
Malone
‘…Dr Robert Malone, who developed the mRNA vaccine…’
He did no such thing. More than 30 years ago, he did some pioneering work introducing mRNA into living cells, but he cannot by any stretch of the imagination be called the inventor of mRNA-based Covid vaccines or any other modern mRNA vaccines.
Many people contributed to the mRNA vaccines we know today, but if there’s a Nobel Prize in it, it will likely go to doctors Katalin Karikó and her collaborator Drew Weissman.
Malone is, however, very bitter that he hasn’t received the credit he feels he deserves. So is his wife. If he really did invent mRNA vaccines, one would expect him to be celebrating their glorious success and demanding a Nobel Prize. Instead, he is waging a war against them with largely baseless warnings about the supposed dangers of the vaccines. Bitterness would explain that.
‘Ivermectin seems to have a general effect in strengthening the body’s defences against a wide range of diseases.’
No, that is not how ivermectin works. At all.
Ivermectin is believed to have anti-viral properties because it interferes with the ability of RNA-based viruses to replicate. Its anti-parasitic action is also a consequence of direct action against the parasites in question. It does not strengthen the body’s defences at all, and in fact has an ‘almost zero impact on the biochemistry of human beings’.
Annoyance
‘It has been used successfully in large scale in India and South America.’
Actually, only days after Mr. Kenny’s article was published, India removed ivermectin from its Covid clinical guidelines, where it had been listed despite ‘a low certainty of the evidence’. It did the same for another experimental drug that those who fear ‘experimental clot shots’ widely advocate, namely hydroxychloroquine.
That ivermectin had been successful in South America – a claim made by the disinformation group Frontline Covid-19 Critical Care Alliance – is also widely disputed, and like in India, countries like Peru no longer recommend it.
‘I think the Covid-19 vaccines are beneficial but don’t think they should be compulsory.’
They aren’t compulsory, and on this point we agree, albeit for very different reasons.
‘I’d probably take one myself if I hadn’t been annoyed by all the disinformation.’
Annoyance is a very poor, even puerile, reason to reject a potentially life-saving vaccine.
Whichever way you slice it, on the subject of ivermectin I fear Mr. Kenny is sadly misinformed. No wonder, then, that his pharmacist gives him looks of horror whenever he goes to fill his ivermectin prescription.
I would strongly advise choosing a Covid-19 vaccine, instead. Unlike with ivermectin, there is lots of data – including from Discovery Health – to show that vaccines are both effective and very safe.
The views of the writer are not necessarily the views of the Daily Friend or the IRR
If you like what you have just read, support the Daily Friend
Image by Arek Socha from Pixabay