
Discovery recently announced an annual 200% spike in cardiometabolic and cancer claims.
This news came from Guy Chennells, head of product at Discovery employee benefits.
Citing no evidence, Chennells provided a list of likely reasons for this rise to credulous journalists. These suggestions include “long Covid”, a decline in cancer screenings and a general reduction in exercise. That is the boring part.
Far more intriguing is what Chennells didn’t say. There is no mention of the established link between mRNA vaccines and heart injury. It appears Discovery was silent on this, and not one mainstream journalist was informed and interested enough to ask.
The evidence is cogent that Covid mRNA injections have a causal relationship with heart injury. I share just some of this evidence below, with links to my sources. Even ardent cheerleaders for vaccine mandates increasingly – if grudgingly – acknowledge some level of risk. For now, we need not delve into frequency and severity. My sole submission is that it is indefensible to exclude these drugs from any list of plausible causes of the spike in heart injuries.
It is difficult to find an acceptable explanation for Discovery’s failure to mention this link. Several unacceptable ones come to mind. One may be that they are incompetent. Is it possible that this fantastically successful insurer, staffed by some of the best actuaries around, has not read and understood the data? Possible, but unlikely.
Another conceivable explanation is that they refuse to look at the evidence. Recall that this company coerced employees and contractors to take these drugs on pain of losing their livelihoods. That might cause even the most well-meaning mind to instinctively close itself to this evidence. [It is unclear whether they are still pressuring people to take these drugs.]
A third explanation seems most likely. Discovery knows that there is a more than plausible case that mRNA vaccines can and do cause heart injury. And they can’t bring themselves to say so. Imagine having to make this announcement: “We coerced people to take a drug that was only available on an emergency use authorisation (EUA), following a radically abbreviated testing process, and have now been quiet for months about reliable evidence that these potent injections can and do cause heart damage.”
Discovery could clarify things by answering one question: Do you deny that Covid vaccines can and do cause heart injury?
If they deny this, I submit they have a daunting task ahead to debunk evidence to the contrary. But I’d invite that effort.
If they acknowledge it, they ought to issue a correction. Then they can begin squaring up to what they have done.
Of course, severe side effects, including the risk of death, don’t inherently make a drug bad. From paracetamol to chemotherapy, we accept potential harms in return for benefits. That demands we understand the harms and benefits as best we can. Discovery has touted the benefits of Covid shots. Until powerful institutions and people who endorsed and even coerced people to take these drugs engage candidly about their negatives, we are fighting a cold war. Transparency and honesty would be far more productive. This is my invitation to Discovery to go the productive route.
If you’d also like to hear Discovery’s take on the matter, consider signing my petition on Change.org: One question for Discovery Health.
You can read earlier pieces on Discovery’s vaccination policy here and here.
The evidence:
A brief selection of evidence supporting the proposition that Covid vaccines are causally linked with heart injury:
- Here is a review study linking mRNA vaccines with cardiac complications.
Among other things, this study finds “Myocarditis/myopericarditis and pericarditis were the most common adverse events among the 243 reported cardiac complications, post mRNA Covid-19 vaccination”

2. More generally, this study out of Harvard, Oxford, Edinburgh and Johns Hopkins (among others) found that the mRNA vaccines are many times more likely to cause a person of student age serious injury than prevent them from being hospitalised with Covid-19.
Their damning conclusion includes: “University booster mandates are unethical because… expected harms are not outweighed by public health benefits given the modest and transient effectiveness of vaccines against transmission…”
3. It does appear that most heart problems caused by vaccines are mild. However, this systematic review of data from the U.K., USA and European Union/European Economic Area found 0.22% (n=30) of 13,571 Covid vaccine-associated myocarditis or pericarditis events were fatal.
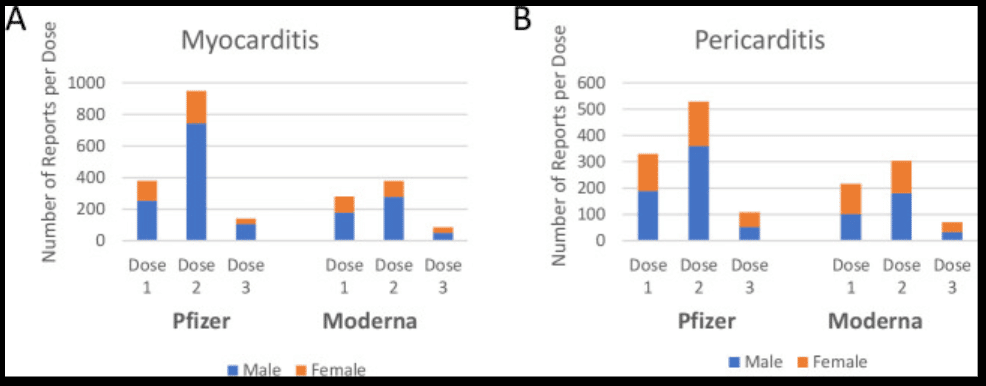
Chart: “Myocarditis and pericarditis events following Covid-19 mRNA vaccination separated by dose data from the Vaccine Adverse Event Reporting System (VAERS; US) reporting system was separated by reaction type; myocarditis (A) and pericarditis (B), vaccine manufacturer and by dose received. stacked bars represent the male and female reports of each condition according to the dose received.”
4. Even the CDC has acknowledged a link between vaccinations and heart inflammation:
“In April 2021, increased cases of myocarditis and pericarditis were reported in the United States after mRNA Covid-19 vaccination (Pfizer-BioNTech and Moderna). Data from multiple studies show a rare risk for myocarditis and/or pericarditis following receipt of mRNA Covid-19 vaccines.”
5. Here is the damning conclusion on the safety of these jabs from a piece in the Journal of Insulin Resistance, “It cannot be said that the consent to receive these agents was fully informed, as is required ethically and legally. A pause and reappraisal of global vaccination policies for Covid-19 is long overdue.”
6. The evidence appears increasingly clear that heart injury depends heavily upon gender, age, brand of vaccine, and the number of doses. Here is a paper concluding “In 18-29 year-old males who received a second dose of mRNA Covid-19 vaccine, attributable risk of myocarditis and/or pericarditis was found to be 5.69 (95% CI: 4.07 – 7.95; p < 0.001) times higher among mRNA-1273 recipients (n = 106) as compared to BNT162b2 recipients (n = 33).” Discovery’s vaccine passport system appears not to have accounted in these differences in risk.
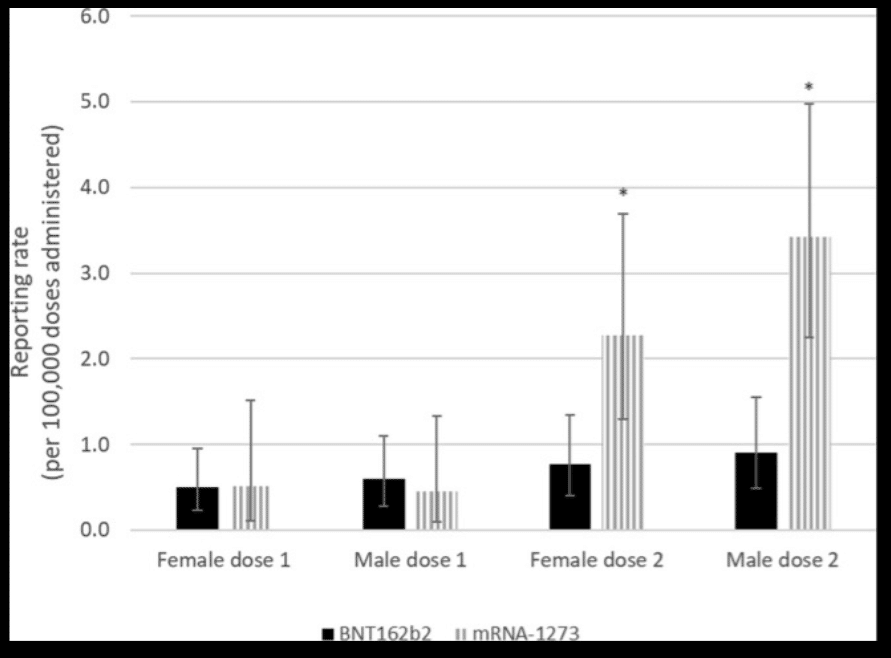
Chart: “Myocarditis and/or pericarditis cases reported in Canada following Covid-19 mRNA vaccination by vaccine type, dose number, and sex in those aged 30–39. *Statistically significant difference.”
7. In this piece in the BMJ’s Journal of Medical Ethics, researchers argue that “Booster mandates in young adults are expected to cause a net harm: per COVID-19 hospitalisation prevented, we anticipate at least 18.5 serious adverse events from mRNA vaccines, including 1.5–4.6 booster-associated myopericarditis cases in males (typically requiring hospitalisation).”
8. Here is a more general discussion about adverse events, including heart injury, associated with mRNA vaccines. Their conclusion, “The excess risk of serious adverse events found in our study points to the need for formal harm-benefit analyses, particularly those that are stratified according to risk of serious COVID-19 outcomes.”
[Image: torstensimon from Pixabay]
The views of the writer are not necessarily the views of the Daily Friend or the IRR
If you like what you have just read, support the Daily Friend