President Cyril Ramaphosa launched the roll-out of a new HIV preventative medicine at the Lillian Ngoyi stadium in Mpumalanga earlier this month that stands to set the country on track to reducing new HIV infections to less than 0.1% by 2032 and getting the HIV pandemic under control around a decade earlier than expected.
South Africa is the first African country and only the third country in the world to register this revolutionary product. Lenacapavir’s registration by the South African Health Products Regulatory Authority was announced at the end of last year.
Around 40 thousand doses are currently being rolled out, but the plan is to place some 400,000 people on preventative therapy over the next two years.
Lenacapavir is indicated for the treatment of multidrug-resistant HIV-1 infection in adults, and for pre-exposure prophylaxis or prevention of HIV infection in both adults and adolescents.
At this stage in South Africa, it is only registered for pre-exposure prophylaxis. If at a later stage its registration is extended, the use will differ, in that it can never be used on its own, as monotherapy, but always in combination with other antiretroviral medicine, in patients with resistant HIV-1 infection or who cannot tolerate the triple therapy in tablet form.
High-risk groups who are encouraged to take up pre-exposure prophylaxis include female sex-workers, men-having-sex-with-men, pregnant and breastfeeding women and adolescent girls.
Lenacapavir marks an important advancement in HIV care and prevention by addressing some of the key issues and difficulties associated with traditional antiretroviral therapy.
False information
In just days after the roll-out, false information is already doing the rounds, including that the injection can cause HIV, or even cancer, or that it is similar to the COVID-vaccine…. Health minister Dr Aaron Motsoaledi has assured Parliament that while the medicine can cause mild side effects like nausea and mild injection-site pain, it cannot cause other diseases. It is safe to use during pregnancy and while breastfeeding, and in adolescents weighing more than 35kg.
The difference between the lenacapavir injection and the vaccine is firstly that it does not contain any viruses, but only a chemical medicine that provides protection against the HIV virus. The way traditional vaccines work is that a small inactivated part of the virus is injected into the body, activating a natural immune response. Antibodies are produced by the immune system, which will then identify and destroy any similar viruses entering the body.
Vaccines like the flu vaccine need to be updated yearly, to adjust for the mutation of the flu virus, or new viruses of the season, while lenacapavir’s chemical formula will stay the same.
If we look at the way the injection works, it is clear why false claims can be disregarded. Lenacapavir is a preventative medication that prevents the HIV virus from infecting the human host cell. It prevents the virus from binding to the human cell-membrane, thus stopping it from entering the human cell nucleus and utilising human DNA to replicate.
New class of medicine
Lenacapavir is a completely new class of medicine in the fight against the HIV virus. In technical terms, it is a capsid-inhibitor, binding to the interface between capsid subunits, altering the capsid stability and function, ultimately preventing integration with the host genome. It works on multiple levels, also preventing viral replication by inhibiting the assembly of the capsid and disrupting the viral core, preventing maturation of the virus.
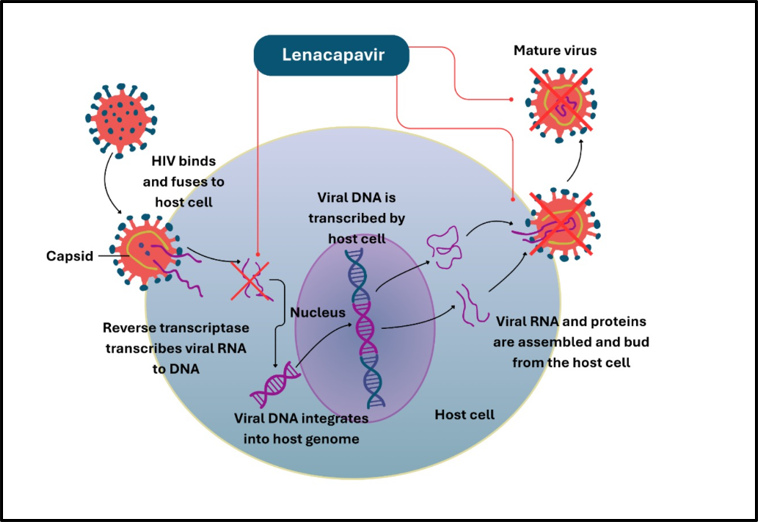
Figure 1: *Multistep inhibition of the HIV life cycle. [Image: Elnieke Bronkhorst]
The depot formulation (or slow-release ‘reservoir’) of lenacapavir is administered with a small needle into the tissues as a low-soluble solution, which is slowly released over six months.
Improve client adherence
The dosing regimen will start with two 300mg oral tablets and two 1.5ml subcutaneous injections (927mg), administered at least 8cm apart on day one. Injection sites include the abdomen or anterior thigh. Two 300mg tablets are given on the second day, whereafter the injection is only required to be administered every six months, which can improve client adherence significantly, and reduce the stigma of visible medication use, improve autonomy, and unstable access to healthcare, and eliminate barriers related to a daily pill burden.
The consistent prevention of the multiplication of the virus can reduce the development of resistance to the treatment of HIV. One aspect of concern is ensuring that clients will return every six months to replenish the depot and ensure sustained protection against the virus. Proper counselling at the clinic where the medicine is administered will be crucial.
Lenacapavir can be considered one of the biggest medical breakthroughs in years for South Africa’s fight against HIV.
Even with the successes of its antiretroviral therapy, South Africa still has a new HIV infection rate of over 200,000 individuals over the age of two every year. Clinical studies with lenacapavir showed that it can be up to 100% effective in preventing new infections.
Lenacapavir is not a cure for HIV, and its use as a prophylactic agent should be in addition to comprehensive HIV prevention strategies, including regular testing and safe-sex practices.
But provided the medicine is rolled out effectively around the country, and that sufficient doses are available, lenacapavir could reduce new HIV infections to less than 0.1% by 2032, and help get the HIV pandemic under control around a decade earlier than expected.
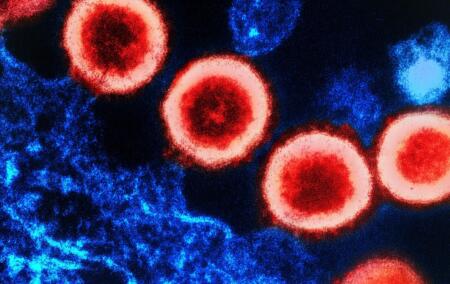
[Image: Transmission electron micrograph of HIV-1 virus particles (red) replicating from the plasma membrane of an infected H9 T cell (blue). Image captured at the NIAID Integrated Research Facility (IRF) in Fort Detrick, Maryland. By NIAID – HIV-1 Virus, CC BY 2.0, https://commons.wikimedia.org/w/index.php?curid=128669911].
The views of the writer are not necessarily the views of the Daily Friend or the IRR.
If you like what you have just read, support the Daily Friend